Contents
Overview
The classification of nerve injuries provides a critical framework for understanding the severity, predicting outcomes, and guiding treatment strategies for damage to the peripheral nervous system. Pioneered by figures like Sir Geoffrey Seddon in 1943 and Sunderland in 1951, these systems categorize injuries based on the structural integrity of the nerve. The lowest grade, neurapraxia, involves temporary disruption of nerve conduction without anatomical damage. Axonotmesis signifies damage to the axon itself while the surrounding connective tissue sheath remains intact, allowing for potential regeneration. The most severe form, neurotmesis, involves complete severance of both the axon and its surrounding connective tissues, necessitating surgical intervention for any hope of functional recovery. These classifications remain foundational in neurology and neurosurgery, influencing diagnostic approaches and therapeutic decisions worldwide.
🎵 Origins & History
The systematic classification of nerve injuries emerged from the urgent need to make sense of battlefield trauma during World War II. Sir Geoffrey Seddon, working at the Royal National Orthopaedic Hospital in London, first proposed a three-tiered system in 1943, distinguishing between neurapraxia, axonotmesis, and neurotmesis. This groundbreaking work was later expanded and refined by Sunderland in 1951, who detailed the histological changes associated with each grade and introduced a five-grade system that provided even greater granularity regarding the degree of connective tissue damage. These early classifications, born from clinical necessity, laid the groundwork for modern peripheral nerve surgery and diagnostic protocols, influencing generations of neurologists and surgeons.
⚙️ How It Works
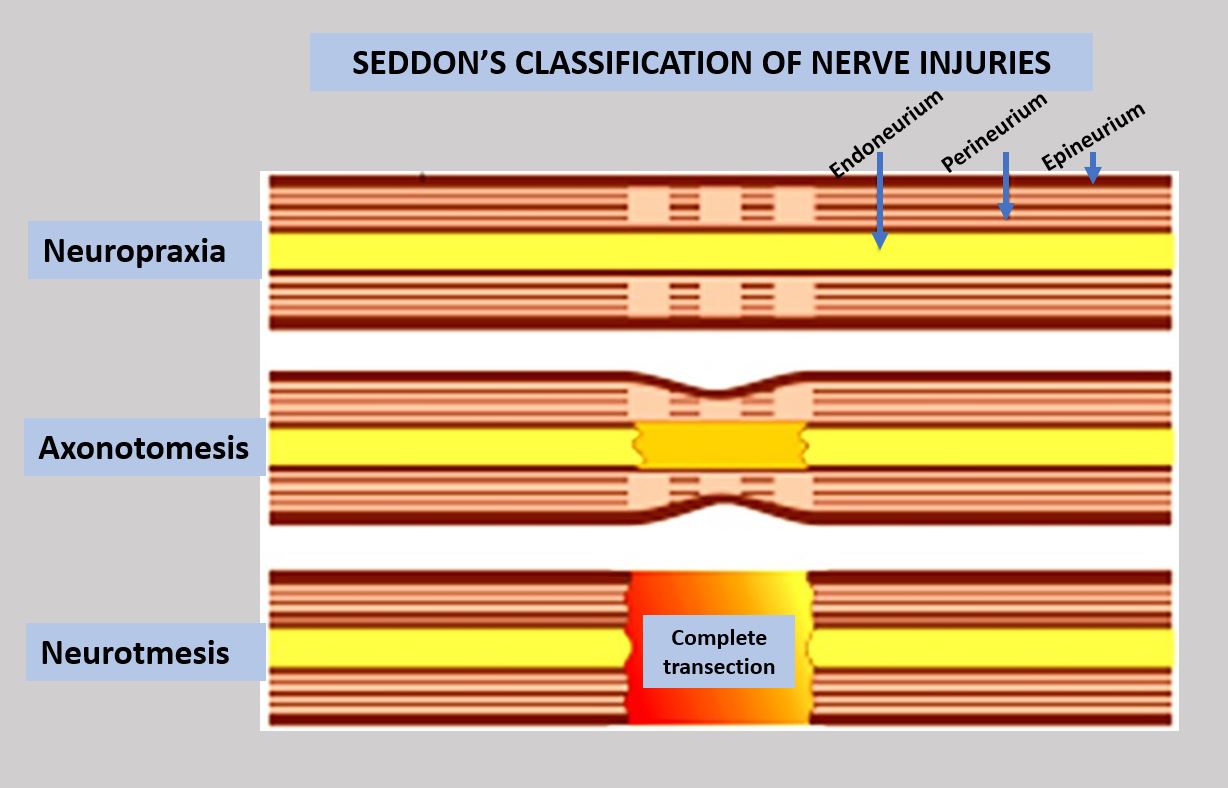
The Seddon and Sunderland classifications categorize nerve injuries based on the extent of structural damage to the nerve fiber and its supporting connective tissues. Neurapraxia, the mildest form, involves a temporary block in nerve conduction, often due to compression or contusion, with no anatomical disruption; nerve function typically returns spontaneously within weeks or months. Axonotmesis, a more severe injury, involves damage to the axon itself, but the endoneurium, perineurium, and epineurium—the nerve's connective tissue sheaths—remain intact. This allows for potential regeneration, though it is often slow and may be incomplete. Neurotmesis represents the most severe injury, characterized by complete transection of the nerve, including both the axon and all surrounding connective tissues. For neurotmesis, surgical repair is necessary for functional recovery.
📊 Key Facts & Numbers
Estimates suggest that peripheral nerve injuries affect a significant number of individuals annually, with a portion requiring classification to guide treatment. Seddon's original classification, proposed in 1943, identified three main grades, while Sunderland's subsequent 1951 work elaborated on these, proposing five distinct grades of severity. For neurotmesis, surgical repair success rates can vary widely, with functional recovery rates reportedly between 30-70% depending on the nerve and the quality of the surgical intervention by specialists at centers like the Mayo Clinic.
👥 Key People & Organizations
The foundational work on nerve injury classification is primarily attributed to Sir Geoffrey Seddon, a British surgeon whose 1943 publication established the initial framework. His contemporary, Sunderland, an Australian anatomist and surgeon, significantly expanded upon Seddon's concepts in his 1951 monograph, providing detailed histological descriptions and a more granular grading system. Key institutions like the Royal National Orthopaedic Hospital in London and the University of Melbourne were instrumental in the research and dissemination of these early classifications. Today, organizations such as the American Academy of Neurology and the World Federation of Neurosurgical Societies continue to refine diagnostic and treatment guidelines informed by these historical classifications.
🌍 Cultural Impact & Influence
The Seddon and Sunderland classifications have profoundly shaped the discourse and practice within neurology and neurosurgery. They provided a common language for clinicians and researchers, enabling more consistent reporting of outcomes and facilitating the development of standardized treatment protocols. The clear distinction between reversible conduction block (neurapraxia), recoverable axonal damage (axonotmesis), and irreversible severance (neurotmesis) allowed for more accurate prognostication, influencing patient expectations and therapeutic aggressiveness. This framework has been a cornerstone in medical education, appearing in countless textbooks and lectures on neuroanatomy and trauma care for decades, solidifying its place in the medical canon.
⚡ Current State & Latest Developments
Current advancements in diagnostic imaging, such as high-resolution ultrasound and MRI, are increasingly complementing clinical examination in assessing nerve injury severity, sometimes offering real-time visualization that can refine the application of Seddon and Sunderland grades. Researchers are also exploring electrophysiological techniques, like EMG and nerve conduction studies, to provide more objective measures of nerve function and regeneration progress, potentially leading to more dynamic classifications. Furthermore, the development of nerve conduits and bioengineered scaffolds by companies like AxoGen aims to improve outcomes for neurotmesis injuries, pushing the boundaries of what's possible beyond traditional surgical repair.
🤔 Controversies & Debates
A persistent debate revolves around the precise delineation between Sunderland's grades II and III, particularly in cases of partial axonotmesis where endoneurial damage is present but the perineurium remains largely intact. Some argue that the five-grade Sunderland system, while detailed, can be overly complex for routine clinical application, leading to inter-observer variability. Consequently, a return to the simpler three-tier Seddon classification is sometimes advocated for its ease of use, despite its reduced granularity. The efficacy of surgical intervention in severe axonotmesis and the optimal timing for such interventions also remain subjects of ongoing clinical research and discussion among neurosurgeons.
🔮 Future Outlook & Predictions
The future of nerve injury classification may see a move towards more objective, data-driven systems that integrate imaging, electrophysiology, and molecular markers. The development of AI algorithms capable of analyzing complex diagnostic data could lead to highly precise injury grading and personalized treatment recommendations. Advances in regenerative medicine, including stem cell therapies and gene therapy, may also necessitate new classification paradigms that account for the potential for enhanced biological repair, moving beyond purely structural assessments. The ultimate goal is a classification system that not only predicts outcome but also directly informs the most effective, personalized therapeutic strategy.
💡 Practical Applications
The primary application of nerve injury classification lies in guiding treatment planning for patients presenting with peripheral nerve damage. For neurapraxia, conservative management involving rest and physiotherapy is typically sufficient. Axonotmesis often requires careful monitoring for signs of regeneration, with surgical exploration considered if recovery stalls. Neurotmesis, however, almost invariably necessitates prompt surgical intervention, such as nerve grafting or nerve transfer, to bridge the gap and facilitate axonal regrowth. These classifications are also crucial for medical malpractice assessments, research studies evaluating treatment efficacy, and the design of rehabilitation programs by physical therapists.
Key Facts
- Category
- science
- Type
- topic